
No category
Dr. Kirkilionis – “A baby wants to be carried”: considerations when buying a baby carrier or baby sling
Considerations When Buying a Baby Carrier or Baby Sling

When judging different baby carriers, baby slings, baby packs, baby tubes, and kangaroo carriers, we prefer carriers that allow baby to sit up straight and face toward the baby-wearers chest.
The residue of harmful chemicals is certainly the first deciding factor, and research on this topic can be found in the Oeko-Test (ecological testing report). You should also examine the baby carrier to ensure that it supports a particular leg position of the child.
The following guidelines will help you evaluate various baby carriers.
Leg Position
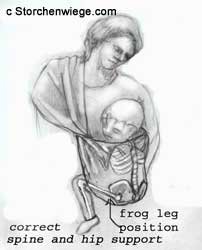
The baby sling should be manufactured to allow the babys legs to be up at least at a 90% angle, more if possible. This legs-up position provides the most support. In order to achieve this position, stretching of the babys legs must be inhibited by another cover or by the crotch base. The cover runs between the babys thigh and along the buttock of the child, and should be wide enough to reach into the popliteal fossa, the hollow or back of the knee.
Baby will automatically pull up the legs into the
correct position when lifted up.

Back Support
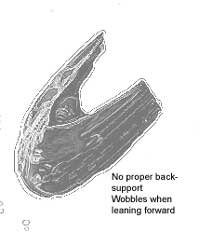
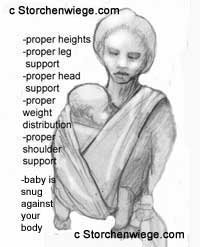
The back of the baby carrier should be wrapped tightly around the baby, providing support as he or she sits straight up in the carrier. The baby should be snug against the parent in an upright positionthis prevents the child from slouching over while sleeping
 Head Support
Head Support
The back of the baby carrier must reach above the babys head. If the carrier is snug, this provides stability to both sides of the head and prevents the head from falling backward or sideways. Tiny infants lack sufficient control of their heads, so this is especially important when your baby is young. As your baby grows, this is only important for when your child is napping.
Adjustability
A baby carrier should, in the cumulative time you plan to carry your child, be adjustable to the changing physical conditions of the baby.
Baby Carriers
Baby carriers are very easy to handle, however, quality varies between manufacturers so you should choose carefully. The most important considerations are correct leg position, sufficient back support, and stabilization of the head.
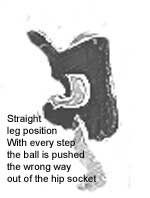
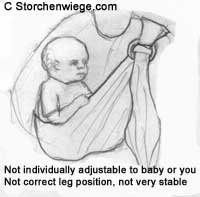
You should first check the leg position of your baby; most baby carriers do not ensure the correct positioning. Some carriers have openings where the babys thighs hang almost straight down. This design does not provide adequate support. In some cases, a squatting leg position is not only impossible, but in the face-to-face orientation, the thighs and knees of the child are pressed up against the adult. With each step of the baby wearer, the childs knees are pushed backward. When this happens, the additional pressure from the childs thighs increases the amount of stretching on his or her hip joints.
When looking at tube slings or ring slings, watch for slings that are too short. The entire bottom of the sling, even when used with a four month old infant, hardly reaches up underneath the shoulder blades. With most of these slings, the suggested age is 3-4 months, however, even at that age these types of slings do not stabilize the back and shoulders sufficiently. Although these carriers seem practical, they simply do not offer your baby sufficient support, especially on prolonged walks.


Wraparound Style Baby Slings
You can certainly make your own sling if your child will only be in it for a short period of time. However, it is often difficult to find a usable, proper material that assures your childs proper sitting position (for more than 15 minutes.) This is also true of many wraparound style baby slings on the market. To find more information, refer to the Oeko-Test article.
Other Considerations
Fabric should give in the horizontal and diagonal directions, in warp and woof.
Fabric folds have to be tightened frequently or re-tied when carrying your child for any length of time.
Diagonal elasticity is the ultimate feature that characterizes a high-quality baby sling. The fabric must not stretch too little or too much.
Wrap the baby tightly to ensure the proper support of his or her posture. After tying the knot and taking a few steps, every loose fold and crease must be tightened in order for the baby sling to embrace your babys body completely.
Make sure the material is not too stiff. When material is stiff and does not stretch at all, it becomes challenging to tie the knot and position the baby correctly.
The after-tying tightening of the creases and folds can be troublesome and time consuming; one crease might be too loose, another too tight for your child. If your baby moves during this process, the babys positioning might be off and the fabric wont evenly embrace your babys body.
Make sure the material is not too stretchy. When the material is loose, any movement from the baby causes the sling to lose its shape.
Qualities of Good Baby Slings
A Firm, Non-Stiff Fabric
Good baby slings are known for their intricate, sophisticated weaves. Sheet-like, cotton fabric does not provide enough firmness and diagonal stretch. Proper threading of twined threads provides both the necessary firmness and stretch.
The fabric must not be too smooth or the knot will gradually give. Conversely, when fabric is too rough, its nearly impossible to retighten the different fabric folds and strands.
For some carrying positions, the baby will slide into a previously tied baby sling. However, if the fabric is too rough, the child can hardly slide, and the babys clothing will cling to the fabric.
Thinner fabrics cut whenever they crease and the folds bunch together. This is most apparent in the sling edges, but also where the folded fabric supports the hollow of the childs knee and along the wearers shoulders. When your babys legs fall asleep, his or her protests should not be surprising, so finding the right fabric medium is important.
Stitching and Pattern
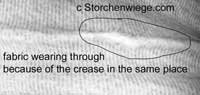 The edges should have a double hemline. Simple-weaved edges wear out quickly, give too much, and stretch easily.
The edges should have a double hemline. Simple-weaved edges wear out quickly, give too much, and stretch easily.
Slings with different colored stripes are the most suitable. All tying methods require you to re-tighten single fabric folds and strands. If the stripes are symmetrical, it is much easier to follow the stripes up the carriers back for re-tightening. (Finding the right fabric fold is not always easy, especially in those positions where the baby sling crosses the baby wearers back, and is then brought to the front again.)
You can, if you own a solid colored baby sling, help yourself by lengthwise stitching different colored threads into your baby sling. Some tying methods have to be retied for each use, so you need the middle as guide. If you have to re-tie for each use, mark the middle with a noticeable thread.
There are many differences and quality levels between baby slings. For more information, we recommend consulting with experienced baby wearers or referring to the Oeko-Test magazine. Keep in mind that even high-quality baby slings wear over time, however, they will not quickly stretch out of shape (requiring you to retie frequently to properly support your child.)
Additional Information
You can often find slings that arent really slings, but are derived from them or copy one of the wraparound sling tying methods.
For example, there are carrying tubes for the hip carrying position. Picture the baby sling Nr 28 (p140) as a tube. This sling is not tied, but it is sewn together. It is not adjustable in size nor can it be adjusted to fit an individual babys physical needs. If these types of slings are suited for any use, they would only be used for older children who can stabilize their backs by themselves; these definitely do not provide adequate support for smaller children. Smaller children need more support from a parents body so that they dont slouch over.
Tube Slings
There are also tube slingsbaby carriers that only use one shoulderfor the front carry. These slings provide limited adjustability, often leaving too much space between the carrier and the child, and do not support the baby sufficiently. I cannot recommend any of the tube slings I am familiar with.
Some baby carriers, which look like a tube that is opened lengthwise, can only be placed over one shoulder and the head. (This is like the already tied, wraparound baby sling in the hip carry.) These carriers are not adjustable due to the narrowness of the fabric. When using them to cradle carry the child in front of the body, some of the fabric strands and folds cannot be tightened individually and can become loose. If you are carrying the baby in an upright position, this is a major drawback because this kind of baby carrier does not provide enough back support. Do not use this style of baby carrier until your child can sit safely unassisted.

 There are also baby slings that support the sideway hip seat or hip carry. For ease of use, these slings are manufactured with rings. The adjustability and overall fit is not as flexible as the wraparound-style sling.
There are also baby slings that support the sideway hip seat or hip carry. For ease of use, these slings are manufactured with rings. The adjustability and overall fit is not as flexible as the wraparound-style sling.
Often in the area of the babys seat, the pouch has only one strap attached. The strap runs diagonally across the back and chest and over the shoulder (like the wraparound style sling in the sideways hip carry.) You can shorten the sling by pulling on the strap; however, the shortening effects are limited: this affects the whole baby carrier, not just the area on your back.
It is rare that tube slings allow you to tighten individual fabric strands. The fabric strands and folds cant be individually adjusted, and therefore, do not tightly embrace the childs back. The parent supports the child with only a small part of the shoulders, which can lead to pain and difficulty carrying the child.
Often the cradle variation is acceptable, although the shoulder strap is located directly on the shoulder muscle. The sling pulls directly on this muscle, instead of distributing the babys weight across the entire shoulder.
Any upright carrying positions in the aforementioned baby carriers should be carefully examined. Most lack the ability to tighten the fabric strands, as mentioned previously, and the ability to ensure the necessary firm back support.
All carriers should also be carefully examined even if they are constructed along the lines of the wraparound style sling (with a square or rectangular piece of fabric), and include precise tying instructions (or buckles or rings.)
Here too, only a small area of the parents shoulder should bear most of the weight. Often, the babys leg or shoulder circulation can be cut off by the edges.
So far, I am not aware of any equal alternative, which can even compare to the versatility, individual adjustability, and tying varieties provided by the wraparound baby sling.
Tips for Using Your Sling
You should carry your child quite high. This creates a suitable weight distribution. When the childs center of gravity is higher, the posture of the carrier will be better. The babys weight will also be less noticeable or bothersome.
The center of gravity also applies to the distance between you and your child. In other words, the closer and higher you carry the baby, the more evenly the childs weight will be distributed.
If the baby pouch leaves too much room between your body and the baby, the childs weight eventually becomes burdensome. Some baby pouches cant be adjusted very high. This is something you should watch for especially if you are petite.
Carrying your child in front of you is more strenuous than carrying him or her on your back. If you have difficulties carrying the child, especially when he or she gets heavier, you should carry the baby on your back especially when walking for long periods of time.
IMPORTANT: Do Not Face Your Baby Outward
Dr. Kikilionis describes the following incident, I observed an infant in the cross carry of a wraparound baby sling, facing away from the mother with his back toward the mothers chest. The leg position was not correct. Sure, the baby can see a lot and usually little ones get quite agile in this position. Events are occurring all around the child that the baby has to observe. I use the phrase has to very deliberately. 
Infants in outward-facing orientations cant turn away from surrounding stimuli. They cant turn inward toward a parents body if it becomes overwhelming. In this position, a child cannot make eye contact with his or her parent to evaluate facial expressions, social cues, and so forth to make assessments of the situation . . . I am not a big supporter of the outward facing method of carrying a child.
Considerations for Buying a Baby Carrier or Baby Sling
 The following tips for choosing a baby carrier were selected from Dr. Eveline Kikilioniss book, A Baby Wants to be Carried. (Currently only available in German: Ein Baby will getragen sein.)
The following tips for choosing a baby carrier were selected from Dr. Eveline Kikilioniss book, A Baby Wants to be Carried. (Currently only available in German: Ein Baby will getragen sein.)
You should examine a baby carrier or baby sling to ensure it meets the following criteria:
1. Fabric. Your first consideration should be how the carrier was manufactured and what materials (look for non-toxic dyes) were used. Your baby will spend a lot of time close to the fabric.
2. Leg Position. The legs should be at least pulled up to a 90 degree angle. This is only possible if the baby sling crotch piece is wide enough so that it will reach to your babys hollow of the knees.
3. Back Support. The back of the carrier needs to support the babys back, so that he or she is not slouching excessively while in the upright position. It needs to be supportive enough that even when your baby is asleep his/her body is tightly secured to your body.
4. Headrest: The back of the carrier needs to reach over the babys head, on all three sides, to keep the head from falling backwards or sideways. (This is very important as long as the infant cant keep his/her head up. As your child grows larger, this is important only when he or she takes a nap.) Make sure the head rest is sturdy and doesnt fold back when pushing on it with your hand.
5. Shoulder Support: Carriers supported by both shoulders with wide straps are best to eliminate back problems for yourself. Carriers that are only supported by one shoulder often worsen the slight scoliosis that most people have.
6. Growth. Your baby is growing fast. Most baby slings are outgrown by 3-9 months. Choose one that will grow with your child.
7. Adjustability. Pick a carrier that can be adjusted to you and your babys needs. Babies carried too low experience pressure pushing their legs back with every step you take (putting too much strain on the hip joints and encouraging hip dysplasia.)
8. Facing in. Only choose a baby carrier that allows your child to face you – never out. Not only does a child need support to hold the leg in a 90 degree angle, there are also too many events going on around your baby. A baby has no way to exclude himself from the environment by turning his head away and towards you. Healthy sleep is difficult for a baby who is facing outward.
9. Heat. Many carriers are made of Nylon. Find one that allows airflow to reach your baby. Any non-breathable fabric will encourage a rash on your babys skin when being carried in hot weather or for an extensive period of time.
10. Hips. When carrying the baby in an upright position, the baby’s hips should always be straddled around the wearer’s body. The legs should be pulled up at a 90 degree angle. The legs are pulled up to support the babys body and balance. When the baby’s knees are pulled up to a 90 degree angle, the baby’s legs are spread between 90 and 120 degree angle around the wearer’s body. This agrees with the babys anatomical make up and supports proper hip development. Most importantly, babies should not be worn facing out.
Hip Dysplasia
Explaining Hip Dysplasia
The femur (thighbone) is the longest and strongest bone in the body. Proximally, the femur has the following: head which fits in the acetabulum of the coxal bone (hip socket) greater and lesser trochanters which provide a place of attachment for the muscles of the legs and buttocks; linea aspera, a crest that serves as a place of attachment for several muscles.
Ball-and-Socket Joints
In the ball and socket joints, the ball-shaped head of one bone fits into the cup-shaped socket of another. Movement in all planes is possible, as well as rotation. The shoulder joint and hip joint are examples of this type.

Risk Factors: Common risk factors include female child, firstborn child, breech birth, large baby, low amniotic fluid, family history. But sometimes every one of these factors is absent, and the baby is still affected.
Acetabulum: The area on the pelvis that is capable of becoming a hip socket. In newborns this area is cartilage, as the child matures this area will ossify or harden into bone. Sometimes also called the area of triradiate cartilage because three bones come together to form the acetabulum.
Hip Dysplasia can be either congenital (CHD) or developmental (DDH) and occurs when the top of the femur (leg bone) is not properly located in the hip socket or not located where the hip socket is expected to develop. Hip dysplasia in humans is normally diagnosed in babies. Statistically, girls have a higher incidence of hip dysplasia than boys. There are a variety of treatments that are used depending on the age of the child and the severity of condition.
Hip Dysplasia in short
Hip dysplasia is a comprehensive term that has been used to include a spectrum of related developmental hip problems in infants and children, often present at birth. Your doctor may have used one of the following diagnoses for your child instead:
* Congential hip dislocation – where the hip is frankly dislocated at birth
* Congential dislocatable hip – where the hip is in place at birth, but dislocates fully when stressed
* Congenital subluxatable hip – where the hip is in place, but dislocates partially when stressed
* Acetabular dysplasia – where the hip socket is shallow and remains shallow, so that the hip is unstable.
* Developmental dysplasia (or dislocation) of the hip – a more recent term, to reflect the fact that there are cases that have apparently normal hips at birth, but develop the problem in the first year of life.
At age one, the affected child may present with a limb. Unfortunately, pain is not a problem in the child, hence it is easy to miss the diagnosis. However, by the time the patient becomes an adult, arthritic changes will occur, and pain will set in.
How do you prevent it?
It is difficult to prevent something the cause of which is still quite elusive. However, it is well known that in cultures that practice infant swaddling and using cradle boards to carry their babies, the incidence of hip dysplasia is very high. On the other hand, cultures that carry their babies astride the mothers=s backs have a low incidence of hip dysplasia. Hence it appears logical to discourage putting the baby=s legs in the extended position, and encourage keeping the baby=s hip spread apart.This latter position places the head of the femur (the ball) agains the acetabulum (the socket), and encourages deepening of the socket.
Developmental Dysplasia of the hip
Developmental Dysplasia (ongoing) process, involves the abnormal formation of the hip joint occurring between fetal life and maturity as a result of instability
Hips that are found normal at birth (and even in the first few months of life) can subsequently be found to be abnormal later. This cannot be overemphasized! The best orthopedist in the world can be fooled by the initial hip exam. We cannot be complacent about your child=s hip stability and development.
If an abnormal hip remains untreated, the child will develop the long-term complications, including:
* osteoarthiritis
* pain
* abnormal gait
* unequal leg length
* decreased agility
Treatment
If unstable hip is recognized at birth, treatment consists of maintaining the position of the hip in flexion (knee up towards head) and abduction (knee away from the centerline) for about 1-2 months.
(Taken from hip-baby.org, www.orthoseek.com/articles/hipdys.html, and www.Dr. Hull.com)
According to this research the best hip and hip joint position is with the knees up and away from the centerline. Also called the frog leg position.
A Storchenwiege baby sling will give your baby this Acorrect@ position to prevent hip dysplasia or support and help your baby should there be a tendency for hip dysplasia already.
As pain is not felt the same for babies it is crucial that we as adults take precaution and provide the best support for our babies.
We are not aware of studies having been done specifically researching the early baby stages of teenagers and adults with hip/leg problems. It would be interesting to see who was carried in a baby carrier not fit for the correct development of the hip. We believe there to be a connection and urge parents continually to seek the best baby carriers/ slings for the proper development of the baby=s hips, spine, neck, and which overall offer the best physical support.