
No category
International Hip Displasia Institute
Summary Statement: Babywearing is becoming increasingly popular along with the growing interest in Attachment Parenting. Proper infant hip position while babywearing is especially important because the period of time for babywearing is usually longer than baby transport. For information about baby transport, please refer to the IHDI Educational Statement regarding baby carriers, car seats, swings, walkers and other equipment. When proper hip position is maintained while babywearing, there may be substantial benefit for natural hip development. The Spread Squat position – also known as the M-Position, or Jockey Position – is recommended with the thighs spread around the mother’s torso and the hips bent so the knees are slightly higher than the buttocks or at the level of the buttocks with the thighs supported. This practice may decrease the risk of hip dysplasia, and should be encouraged in regions with high prevalence of hip dysplasia especially where screening and treatment are insufficient.
Education Statement: Research in the 1950s showed the harmful effects of traditional swaddling and the beneficial effects of babywearing for prevention and treatment of hip dysplasia. C. Stuart Houston, MD produced a documentary film on this topic in 1954. Dr. Houston’s documentary film received limited attention at the time, and was recently uncovered by a member of the IHDI Medical Advisory Board.
As many as one in six newborn babies have mild hip instability at birth, and approximately one per thousand has a dislocated hip. Babies with increased risk include those with one or more of the following: a family history of hip dysplasia, breech position, first born, female gender, prolonged labor and larger babies. Screening for hip dysplasia identifies the majority of babies with hip instability. However, late presentation of hip dislocation continues to occur even in countries with universal ultrasound screening of all infants.1 Newborn hip instability is only part of the problem. A study from Norway reported that 90% of young adult hip joint replacements for dysplasia were never diagnosed as dysplasia during infancy.2This suggests that milder types of hip dysplasia are often undetected, or that hip development is abnormal for most people with adult hip dysplasia.
Cultures where babywearing is common have a low frequency of hip dislocations in babies.3 Whether this is due to the M-carrying position or to genetics is unproven. However, this low frequency is in sharp contrast to high rates of hip dislocation where traditional swaddling is practiced with the hips and knees held straight during early infancy.4
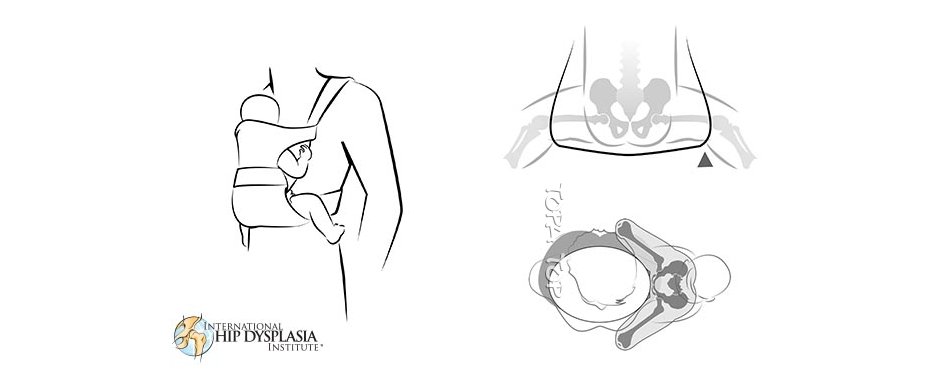
When baby wearing is practiced with each hip in approximately 40° to 55° of abduction and 90° to 110° of flexion, the femoral head – the ball of the hip joint – is pressed evenly into the center of the hip socket. Muscle action of the infant further presses the ball into the socket as the infant moves and clings to the mother.5 This type of muscle activity is beneficial for healthy joint development.6,7
A recent scientific report has provided additional information that back-carrying may decrease the risk of hip dysplasia in Malawi.3 Although this is still controversial, the International Hip Dysplasia Institute supports the conclusion of the authors, who stated, “If a carrying position of infants during early months of development can reduce the incidence of DDH, then a public health initiative promoting back-carrying could have significant world health and financial implications in the future management of DDH and also have potentially huge effects on the timing and severity of development of adult hip arthritis.”
The International Hip Dysplasia Institute supports proper babywearing with the hips in the M-position as a method to encourage healthy hip development.
Sewell M, Eastwood DM. Screening and treatment in developmental dysplasia of the hip – where do we go from here? Intl. Orthop. 2011;35(9):1359-1367.
Engesaeter I, Lie SA, Lehmann TG, Furnes O, Vollset SE, Engesaeter LB,. Neonatal hip instability and risk of total hip replacement in young adulthood. Acta. Orthop. 2008;79:321-326.
Graham S, Manara J, Chokotho L, Harrison WJ. Back-carrying infants to prevent developmental hip dysplasia ans its sequelae: is a new public health initiative needed? J. Pediatr. Orthop. 2015;35(1):57-61.
Mahan S, Kasser JR. Does swaddling influence developmental dysplasia of the hip? Pediatrics. 2008;121:177-178.
Fettweis E. Muscle-mechanical and biomechanical conditions of the squat-seat position in the treatment of infantile dislocation of the hip.[German] Orthop. Praxis. 1991;8 19/91:474-481.
Heegaard J, Beaupre GS, Carter DR Mechanically modulated cartilage growth may regulate joint surface morphogenesis. J Orthop Res. 1999;17:509-517.
Zuscik M, Hilton JM, Zhang X, Chen D, O’Keef RJ. Regulation of chondrogenesis and chondrocyte differentiation by stress. J Clin Invest. 2008;118(2):429-438.
https://hipdysplasia.org/baby-wearing/